
Amol Akhade, Senior Consultant Medical Oncologist and Hemato-Oncologist at Suyog Cancer Clinics and Reliance Hospitals, shared a post on LinkedIn:
“Can dual checkpoint blockade plus trastuzumab overcome resistance in HER2+ MBC?
Fresh insights from the DIAMOND trial suggest: maybe, but not for all.
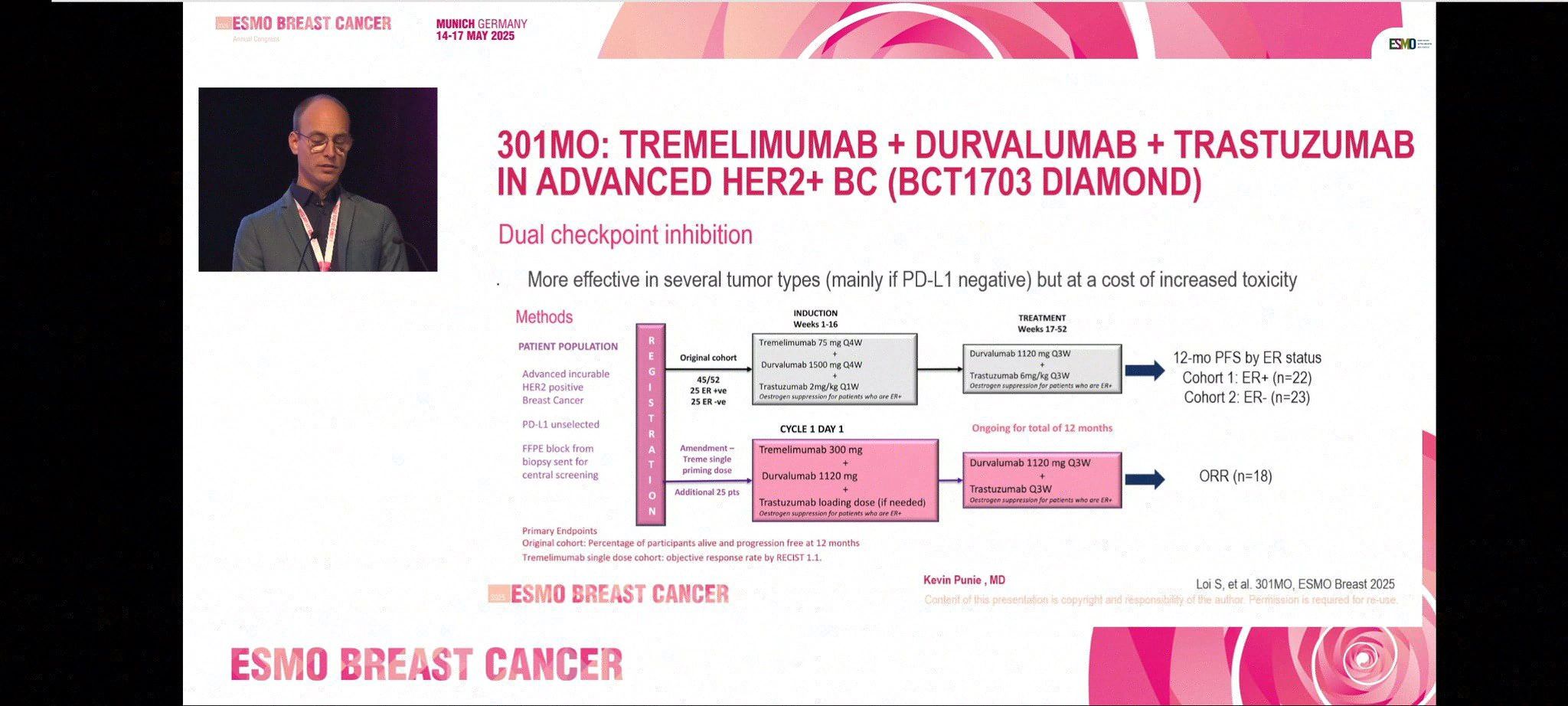
BCT 1703 (DIAMOND) evaluated:
Tremelimumab (CTLA-4) + Durvalumab (PD-L1) + Trastuzumab in trastuzumab-resistant HER2+ breast cancer PD-L1 unselected | ER-stratified | Heavily pretreated
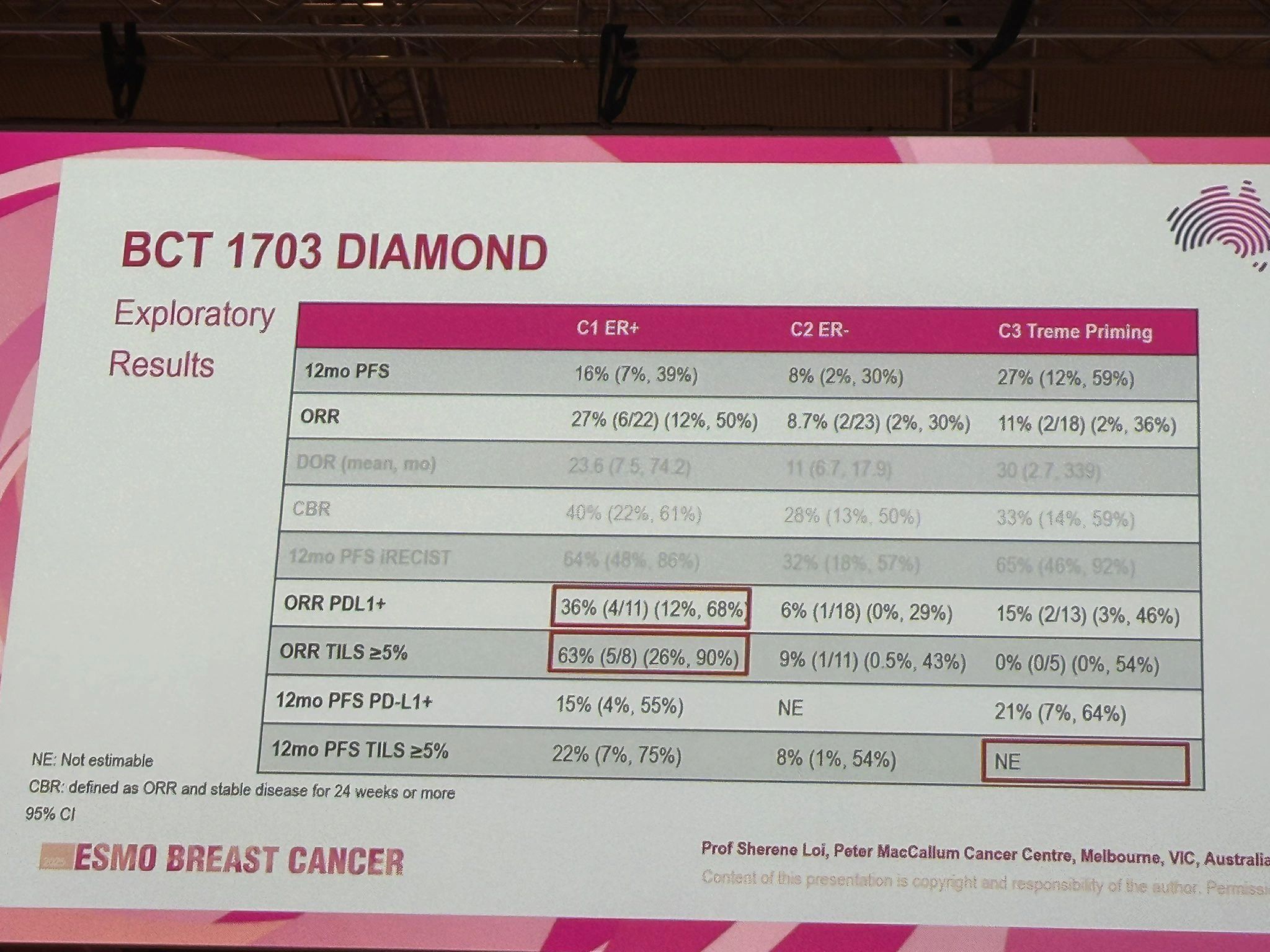
Key Results:
- Cohort 1 (ER+)
- ORR: 27%
- PD-L1+: ORR 36%
- TIL ≥5%: ORR 63%
- DOR: up to 30 months
Cohort 3 (Single priming dose Treme)
- 12-mo PFS: 27%
- Lower toxicity than full-dose tremelimumab
- Activity seen even without high PD-L1 or TILs
What’s exciting?
Durable responses in biomarker-enriched subsets A single priming dose of CTLA-4 blockade may be enough Potential to reduce toxicity without compromising efficacy
But…
- Small sample size (N~20 per arm)
- No comparator (e.g., PD-1 mono or trastuzumab + durvalumab)
- Most patients were T-DXd naïve—future relevance uncertain
- Biomarker response inconsistent across ER groups
Takeaway
Dual ICI + HER2-targeting could benefit ER+, PD-L1+, TIL-high patients—but biomarker-driven selection and comparator-controlled trials are essential next steps.
Single-dose CTLA-4 priming might become a smarter, safer way to use dual ICI in breast cancer.”

More posts featuring Amol Akhade.
{kind=link}
{kind=link}
{kind=link}