
Enrique Grande, Head of Oncology at MD Anderson Cancer Center, shared a recent paper by Thomas Powles and colleagues on LinkedIn published in NEJM:
Perioperative Durvalumab with Neoadjuvant Chemotherapy in Operable Bladder Cancer
Authors: Thomas Powles et al.

The trial involved 1,063 patients to evaluate the impact of adding neoadjuvant durvalumab to chemotherapy for individuals with muscle-invasive bladder cancer. 533 patients were assigned to the durvalumab group, and 530 patients were assigned to the chemotherapy-alone group.
Patients in the durvalumab group received durvalumab plus gemcitabine-cisplatin followed by surgery and more durvalumab, while those in the comparison group received only chemotherapy followed by surgery. The study focused on event-free survival and overall survival as primary and secondary end points.
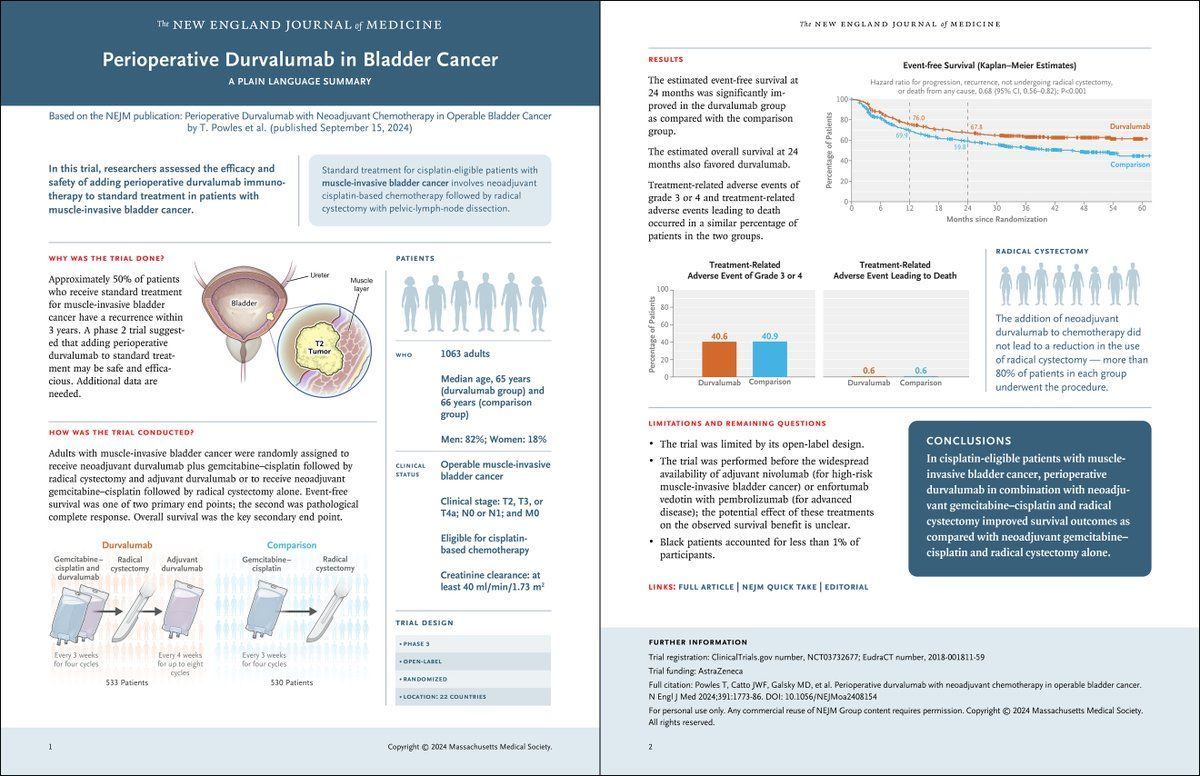
The results showed that patients in the durvalumab group had a significantly higher event-free survival rate at 24 months (67.8%) compared to those in the chemotherapy-alone group (59.8%). This was supported by a hazard ratio of 0.68, indicating a lower risk of progression, recurrence, or death in the durvalumab group. Overall survival at 24 months was also better in the durvalumab group (82.2%) compared to the chemotherapy-alone group (75.2%).
While both groups had similar rates of severe treatment-related side effects (around 40%), the addition of durvalumab did not lead to higher rates of treatment-related deaths, with both groups experiencing 0.6% mortality due to treatment. Radical cystectomy was performed more frequently in the durvalumab group (88.0%) than in the comparison group (83.2%).
This article showed that perioperative durvalumab plus neoadjuvant chemotherapy significantly improved both event-free survival and overall survival compared to chemotherapy alone in patients with muscle-invasive bladder cancer.
{kind=link}